An Education Guide to Help Understand Injury to the Anterior Cruciate Ligament
Dr. Mannarino provides this guide for patients to learn and understand the nature of their injury. We hope this will be helpful as you make decisions regarding your knee.
The Normal ACL
The major role of the ACL is to resist anterior displacement of the tibia (shin bone) on the femur (thigh bone). It is vitally important for participation in twisting, cutting and jumping sports like basketball, football, soccer, volleyball, gymnastics and downhill skiing. (See figure A)
The “Injured” ACL
The patient’s history is significant in making the proper diagnosis. The injury can occur with and without contact as a result of a hard twist or awkward landing from a jump. One third of the patients recall an audible pop at the time of injury. Swelling almost always occurs within 24 hours of the time of the injury and represents blood in the joint. The knee joint has a wide range of disability after the injury from substantial pain with the need to use crutches and a splint to much more mild discomfort, which causes the patient only to walk with a slight limp. (See figure B)
Making the Diagnosis
After taking a proper history, the orthopaedic surgeon can make a definitive diagnosis in most cases by physical examination. An experienced examiner can detect the abnormal sloppiness that occurs in the knee after a tear to the ACL.
Routine X-rays are necessary to rule out any associated bony injury. A magnetic resonance imaging (MRI) scan is often done to substantiate the diagnosis. MRI is helpful to study the meniscal cartilages and subtle bony injury. Many patients feel more comfortable when MRI supports the diagnosis.
Decision Making After Tearing the ACL
Basically, two choices are present after suffering a complete tear of the ACL. The first is to consider an arthroscopic ACL reconstruction using a graft or a tissue substitute. The original ACL cannot be sewn back in place due to its poor healing potential. A replacement for the ACL must be done to achieve predictable success. This alternative requires 4 to 6 months of rehabilitation before return to athletics is possible. The success rate is 95 percent, although many patients still complain that their knee will ache or feel stiff on occasion.
The second alternative is to rehabilitate the knee until the pain and swelling are gone and full strength and mobility have returned. This alternative also necessitates a modification in one’s participation in jumping and twisting sports. Non-jarring sports like swimming, cycling, straight ahead running, and aerobics can be done quite successfully. A period of 4 to 12 weeks is required to rehabilitate the knee if one chooses this alternative.
Those individuals who participate avidly in jumping and twisting sports should consider a reconstruction of the anterior cruciate ligament if unwilling to modify their athletics. Otherwise, continued participation will predictably result in giving out of the knee increasing damage to its structures including the meniscal cartilages and the joint padding. A sedentary individual or one who participates solely in non-twisting sports might be treated with rehabilitation alone. Difficult decisions occur for those individuals who are somewhere in between. In this era of improved arthroscopic techniques, more patients are choosing the surgical route.
The Surgical Procedure
As mentioned previously the anterior cruciate ligament cannot be directly sewn back together because of the nature of the tear. Direct suturing of the anterior cruciate ligament was a procedure that was done some years ago but with very poor success.
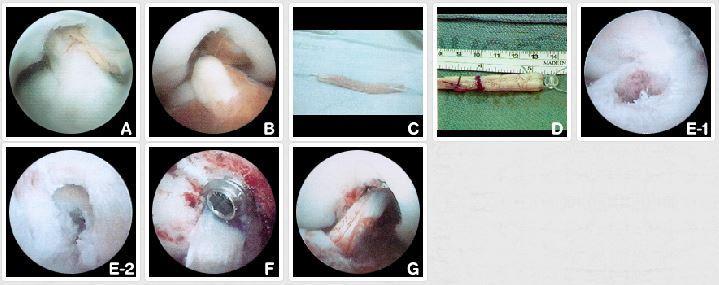
A replacement of the ACL has to be done in order to rebuild the ligament. The patient’s own patella tendon (See figure C) or hamstring tendons (See figure D) can be used as a substitute. Both grafts are used successfully throughout the world. Each has its advantages and disadvantages.
The patella tendon graft heals quickly to the knee and athletes can return to play at 4 months post-op if range of motion and strength have been regained. The patella tendon has a small bone plug on either end of the graft, which allows for secure fixation in the tunnels that are drilled. The patello-femoral mechanism, however, is disturbed some by the harvesting of this graft. Short term, this causes pain and quadriceps dysfunction. Long term problems with the patello-femoral joint have not been unquestionably documented, but this group seems to have more patello-femoral pain.
The initial disability after a hamstring graft is less than after a patella tendon graft. The incision is smaller, and the patello-femoral mechanism is not disturbed. Patients regain control of their extremity easier. The hamstring graft is slower to be incorporated into the bone tunnels and the return to play is usually not permitted until 6 months post-op. The hamstring tendon incorporates more slowly into the knee because this is strictly a soft tissue graft. The soft tissue graft cannot be fixed quite as securely to the knee as a bone/tendon/bone patellar tendon graft. Also, the soft tissue incorporates into the bone of the tunnels slightly more slowly than the bone plugs on either end of the patellar tendon graft. This accounts for the somewhat slower healing process and delayed return to play, compared to the patellar tendon graft.
With either technique the torn ACL is removed. Bone tunnels are made (See figure E) and the graft is fixed to the knee with biodegradable screws (See figure F). Secure fixation allows immediate range of motion and weight bearing. The graft is put into the knee under tension so the abnormal sloppiness in the joint detected after the ACL is torn is eliminated (See figure G).
The Day of Surgery
Surgery can be done on an outpatient or an ambulatory basis. After surgery, the leg is placed in a supportive brace with hinges at the knee that allow range of motion of the knee. A continuous passive motion (CPM) device is used after surgery to begin range of motion of the knee. Emphasis is also placed on straightening or extension of the knee since this is one of the most important aspects of early rehabilitation. A cold pad is usually incorporated into the dressing to help control pain and swelling after surgery.
Postoperative Course
After the patient returns home, he or she needs to stay relatively inactive for the first 5 to 6 days after surgery. This is to help control the swelling. The patient will be seen in the doctor’s office anywhere from 5 to 7 days after surgery. At that time, the dressing is changed, and the patient is allowed to take a shower. Physical therapy will begin 6 to 7 days after surgery.
The patient will go to physical therapy several times a week for approximately an hour. For those patients who are in the student age group, this almost always occurs after school hours. The first week is vital in the initial rehab process and in the control of swelling.
Rehabilitation
Patients are in formal physical therapy anywhere from 6 to 25 visits after surgery. This will depend on how quickly the recovery process is occurring.
After formal physical therapy is over, patients will continue to rehabilitate and strengthen their knee on their own for many months. The first 6 weeks of rehabilitation emphasizes muscle toning, proper gait training and range of motion of the knee. During that first 6 weeks the patient will also begin cycling as well as swimming.
At 6 weeks patients who have obtained good range of motion will begin more vigorous muscle strengthening activities. Somewhere between 6 and 12 weeks after surgery, straight ahead running can be commenced after an appropriate brace has been ordered.
In the 4th, 5th, and 6th months after surgery the patient will gradually come back to activities that involve twisting and turning in preparation for the return to sports. It is usually recommended that the patient come back to sports somewhere between 4 and 6 months after surgery provided that he or she has regained full range of motion and at least 80 percent of their normal strength.
A protective sports brace is used until the patient is 12 to 14 months after surgery since the anterior cruciate ligament that has been implanted in the knee will continue to gain strength in the patient’s knee for 12 to 14 months.
We hope that this educational guide has been helpful to you. This is just one way for us to help you understand the nature of your injury. Obviously this guide cannot substitute for ongoing communication between the surgeon and the patient and their family. We certainly will encourage this throughout the course of evaluation and treatment.
Article by Frank P. Mannarino, M.D.